Anterior Cervical Discectomy and Fusion (ACDF) vs. Anterior Cervical Disc Arthroplasty (ACDA)
Introduction
Cervical spine disorders, including cervical radiculopathy, cervical stenosis, and cervical instability, can cause significant morbidity. Surgical intervention is often required when conservative treatments fail. Two primary anterior approaches are anterior cervical discectomy and fusion (ACDF) and anterior cervical disc arthroplasty (ACDA). This article provides an in-depth analysis of these procedures, their indications, advantages, complications, and long-term outcomes.
Pathophysiology of Cervical Disorders
Cervical Radiculopathy
Cervical radiculopathy results from nerve root compression due to herniated intervertebral discs, osteophyte formation, or degenerative changes in the facet joints. Patients present with neck pain, radiating arm pain, paresthesia, and motor weakness.
Cervical Stenosis
Cervical stenosis is a narrowing of the spinal canal due to degenerative changes, ossification of the posterior longitudinal ligament (OPLL), or congenital factors. This condition may lead to cervical myelopathy, characterized by gait instability, hand clumsiness, and hyperreflexia.
Cervical Instability
Cervical instability occurs due to trauma, inflammatory disorders (such as rheumatoid arthritis), or degenerative disc disease. It can cause abnormal motion between vertebrae, leading to pain and neurological deficits.
Treatment Options
Conservative Management
Physical therapy: Strengthening exercises and posture correction.
Medications: NSAIDs, muscle relaxants, and neuropathic pain medications.
Cervical traction: Reduction of nerve root compression.
Bracing: Short-term immobilization in cases of instability.
Minimally Invasive Interventions
Cervical epidural steroid injections: Reduce inflammation around compressed nerve roots.
Facet joint injections and medial branch blocks: Alleviate pain from facet joint pathology.
Radiofrequency ablation: Provides longer-term pain relief by disrupting nociceptive pathways.
Surgical Interventions
Anterior Cervical Approaches
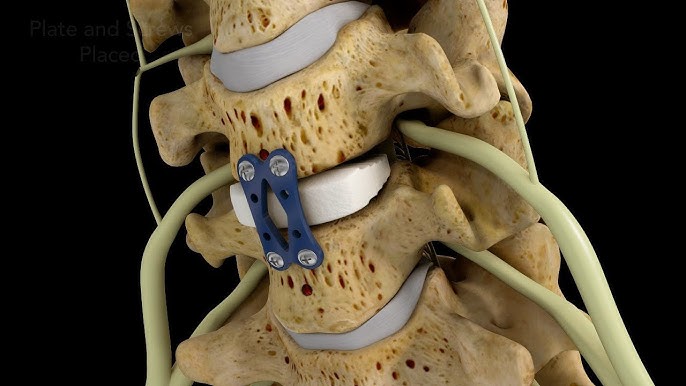
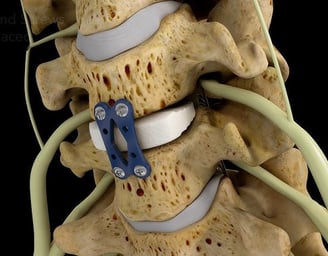
ACDF: Removal of the intervertebral disc and fusion of adjacent vertebrae using a bone graft and/or interbody cage.
ACDA: Replacement of the diseased disc with an artificial prosthesis to preserve motion.
Posterior Cervical Decompression
Laminectomy: Removal of the lamina to relieve spinal cord compression in cases of multilevel cervical stenosis.
Laminoplasty: Expansion of the spinal canal while preserving motion.
Foraminotomy: Enlargement of the neural foramen to relieve nerve root compression.
Indications for ACDF and ACDA
Indications for ACDF
Cervical radiculopathy or myelopathy due to disc herniation or spondylosis.
Instability requiring stabilization.
Recurrent disc herniation.
Failed conservative treatment.
Indications for ACDA
Single-level or two-level disc disease.
Absence of significant facet joint arthritis or instability.
Younger patients with preserved motion segment.
Indications for Posterior Decompression Alone
Multilevel cervical stenosis without significant anterior compression.
Congenital spinal canal narrowing.
Myelopathy with preserved lordosis.
Complications of ACDF and ACDA
ACDF-Specific Complications
Adjacent segment disease.
Pseudarthrosis (non-union of the fusion site).
Dysphagia.
Graft dislodgement.
Hardware failure.
ACDA-Specific Complications
Device subsidence.
Heterotopic ossification leading to loss of motion.
Wear-related prosthesis failure.
Spinal cord or nerve root injury.
Long-Term Considerations
Adjacent Segment Disease (ASD)
ASD is a long-term complication of ACDF, characterized by accelerated degeneration at levels adjacent to a fused segment. This occurs due to increased biomechanical stress.
Progressive Degenerative Changes
Both ACDF and ACDA patients may develop degenerative changes over time.
ACDA has a lower incidence of adjacent segment disease but is not completely protective.
Conclusion
Both ACDF and ACDA are effective treatments for cervical spine pathology. ACDF remains the gold standard for cases requiring stability, while ACDA offers motion preservation and reduced adjacent segment disease. A patient-specific approach should be taken when deciding between these procedures, considering anatomical, pathological, and functional outcomes.
Contact
Schedule your consultation with our expert team.
Resources
info@thebrainandspine.com
123-456-7890
© 2024. All rights reserved.